The term "omega-3" covers three distinct fatty acids with meaningfully different evidence bases:
ALA (alpha-linolenic acid): The plant-based omega-3 found in flaxseed, chia, hemp, and walnuts. The body can convert ALA to EPA and DHA, but conversion efficiency is very low: typically 5 to 10 percent for EPA and less than 1 percent for DHA. ALA has weak independent cardiovascular evidence.
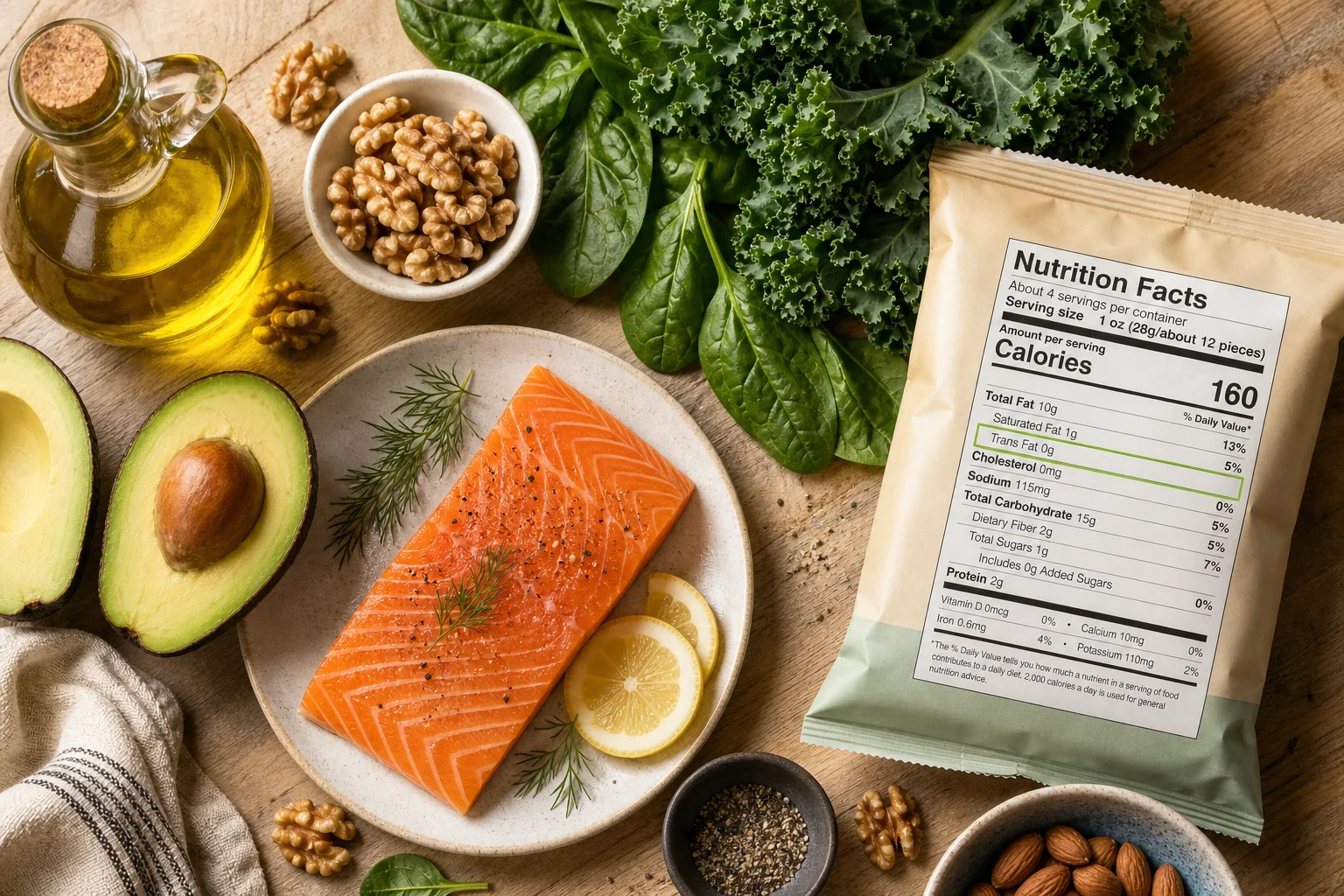
EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid): The marine omega-3s found in fatty fish (salmon, sardines, mackerel, anchovies) and fish oil supplements. EPA and DHA are the biologically active forms with documented cardiovascular effects: triglyceride reduction, anti-inflammatory effects, and plaque stabilization.
FDA allows "excellent source of omega-3" claims for products containing ALA from plant sources, even though these do not deliver the EPA and DHA with clinical evidence. A product labeled "rich in omega-3" may contain only ALA, providing no appreciable cardiovascular benefit.
How to read omega-3 supplement labels: Look for the specific declaration of EPA and DHA in milligrams per serving, not "total omega-3s," which may include ALA. A standard fish oil capsule containing 1,000 mg of fish oil may contain only 180 mg EPA and 120 mg DHA, with the remainder being other fatty acids. High-concentration fish oil provides 500 to 1,000 mg EPA+DHA per capsule.
The prescription drug Vascepa (icosapentaenoic acid, pure EPA at 4 grams/day) showed a 25 percent reduction in cardiovascular events in the REDUCE-IT trial in patients with elevated triglycerides already on statins. This clinical benefit does not extrapolate to standard over-the-counter omega-3 supplements at typical doses.