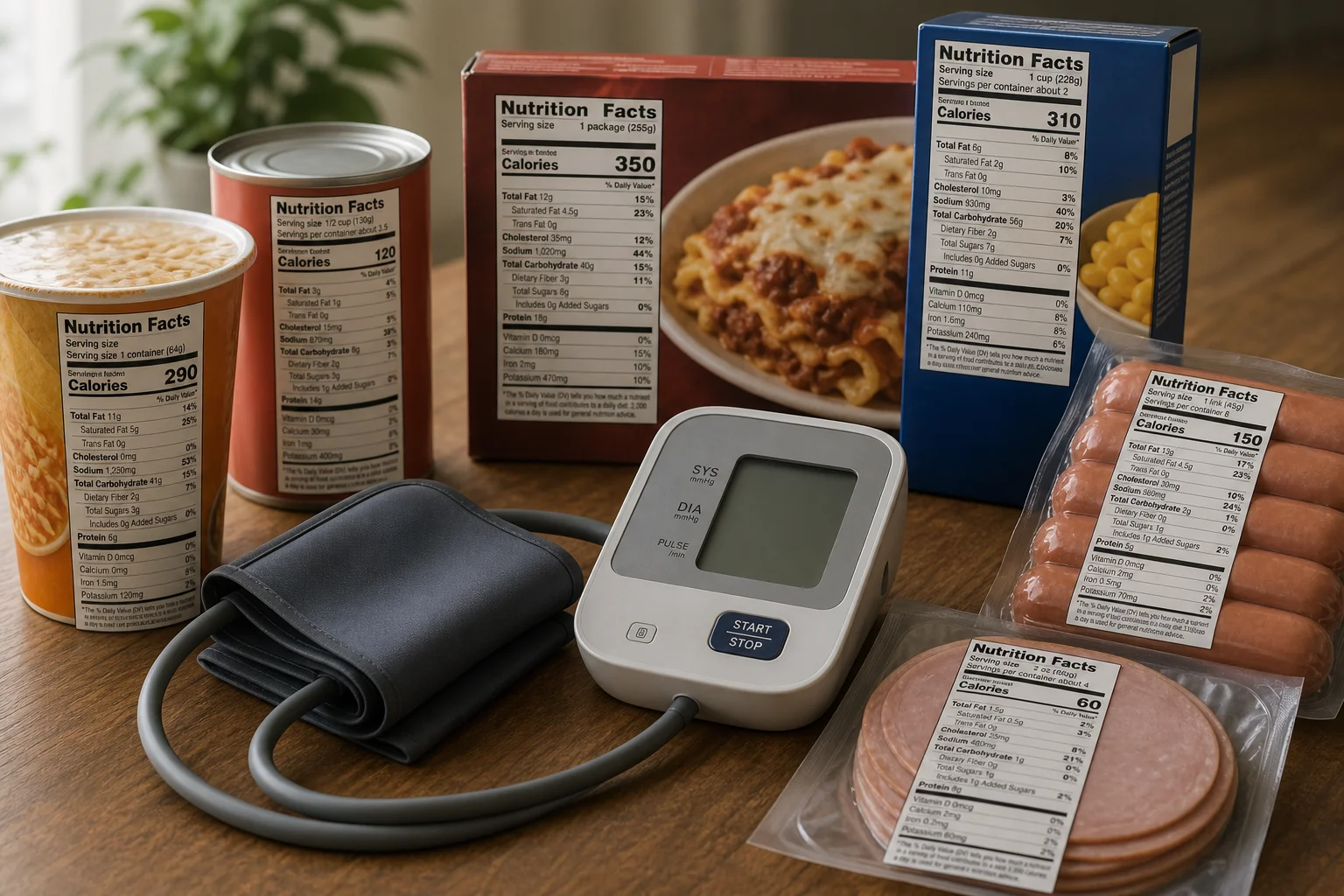
About 70 percent of Americans' dietary sodium comes from processed and restaurant foods, not the salt shaker. Many of these sources are invisible on casual label review:
Bread and baked goods: A single slice of commercial bread can contain 100 to 200 mg of sodium, and bread is the leading source of sodium in the American diet by sheer volume consumed. A sandwich using two slices and deli meat can easily deliver 1,000 to 1,200 mg of sodium.
Cottage cheese: 400 to 500 mg per half-cup serving, more than many processed snack foods.
Canned tomato products: Canned diced tomatoes contain 300 to 400 mg per half-cup. Tomato sauce: 400 to 500 mg. Tomato juice: up to 700 mg per 8 ounces.
Soy sauce and tamari: Standard soy sauce contains approximately 900 to 1,000 mg per tablespoon. "Reduced sodium" soy sauce still contains approximately 600 mg.
Monosodium glutamate (MSG): Contains about 12 percent sodium by weight, compared to table salt at 39 percent sodium. FDA requires MSG to be listed by name in ingredients.
Sodium in unexpected forms on ingredient lists:
- Sodium benzoate (preservative)
- Sodium bicarbonate (baking soda, leavening)
- Sodium citrate (pH control)
- Sodium nitrate / nitrite (curing agent in processed meats)
- Sodium phosphate (stabilizer, common in processed cheese)
- Disodium inosinate (flavor enhancer, often combined with MSG)
- Disodium guanylate (flavor enhancer)
- Sodium alginate (thickener in dairy analogs)
- Sodium lauryl sulfate (in some baked goods)
These forms of sodium do not appear in the overall "Sodium" line on the Nutrition Facts panel alongside table salt, they are all included in that total. But consumers who scan labels for the word "salt" miss them.
Restaurant food: A single restaurant meal frequently contains 2,000 to 3,000 mg of sodium. Menu labeling rules (effective 2018) require large restaurant chains to post calorie counts, but sodium is not required to be disclosed to customers unless specifically requested.