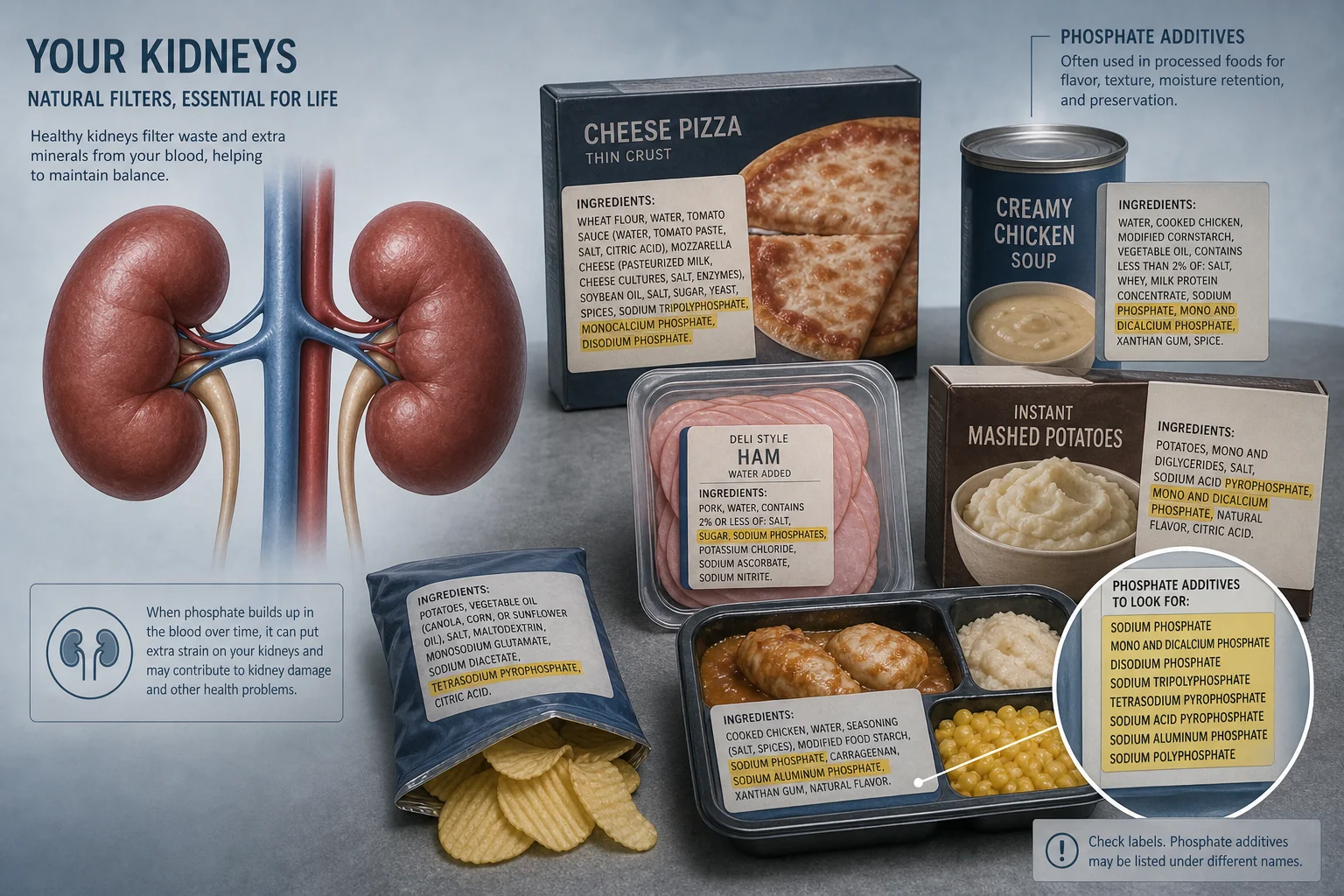
Chronic kidney disease (CKD) affects an estimated 10 to 13 percent of the global adult population, more than 850 million people worldwide. Its dietary management involves one of the most complex intersections of nutrition science and food regulation of any common health condition. Three minerals, phosphorus, potassium, and sodium, all require tight management, and all three hide in processed food in ways that current US label regulations fail to adequately disclose.
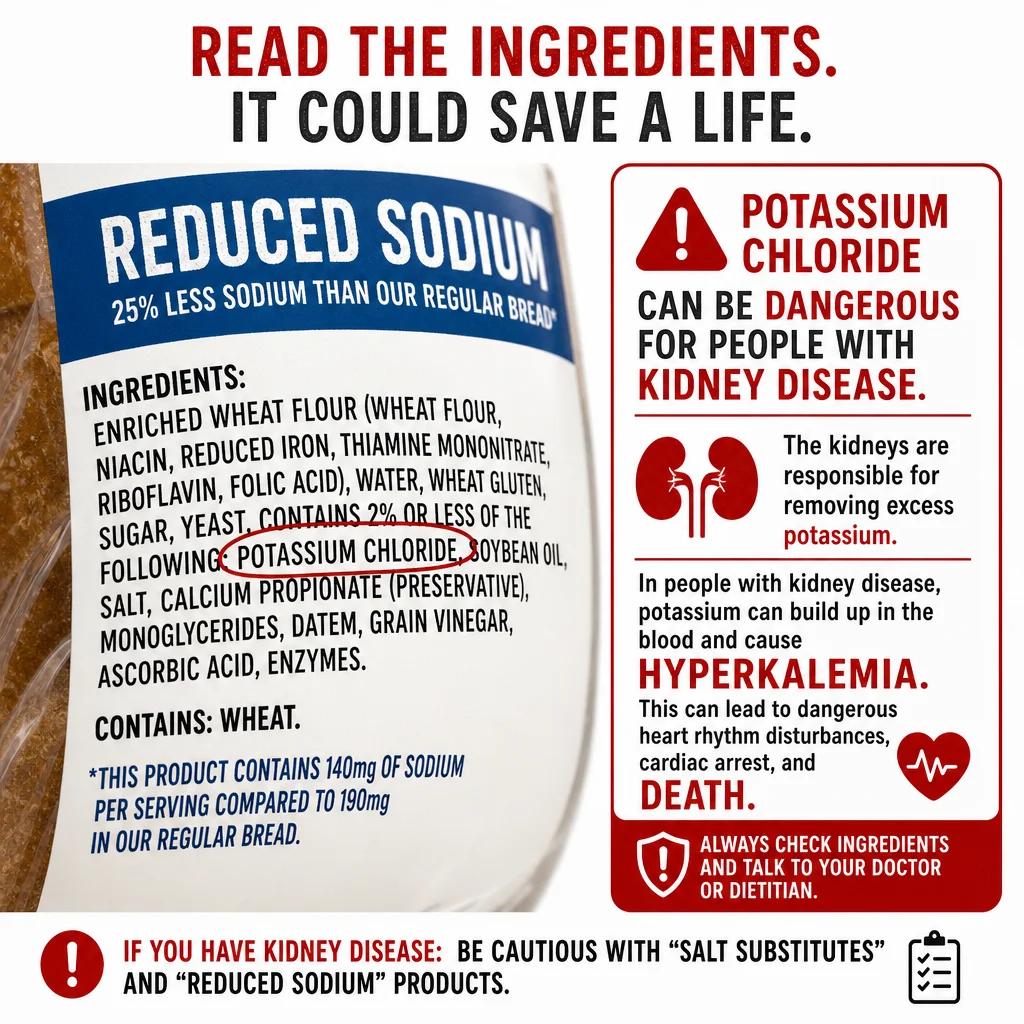
The most dangerous example is potassium chloride. Widely marketed as a "healthy" salt substitute for people managing high blood pressure, it is capable of causing fatal cardiac arrest in patients with impaired kidney function. A 2003 BMJ case report documented a patient with CKD whose potassium level reached 9.7 mmol/L, nearly twice the upper limit of the normal range, after switching to a potassium chloride salt substitute, resulting in two cardiac arrests. The patient survived, but the incident illustrates precisely why kidney disease requires a different framework for reading food labels than any other condition.