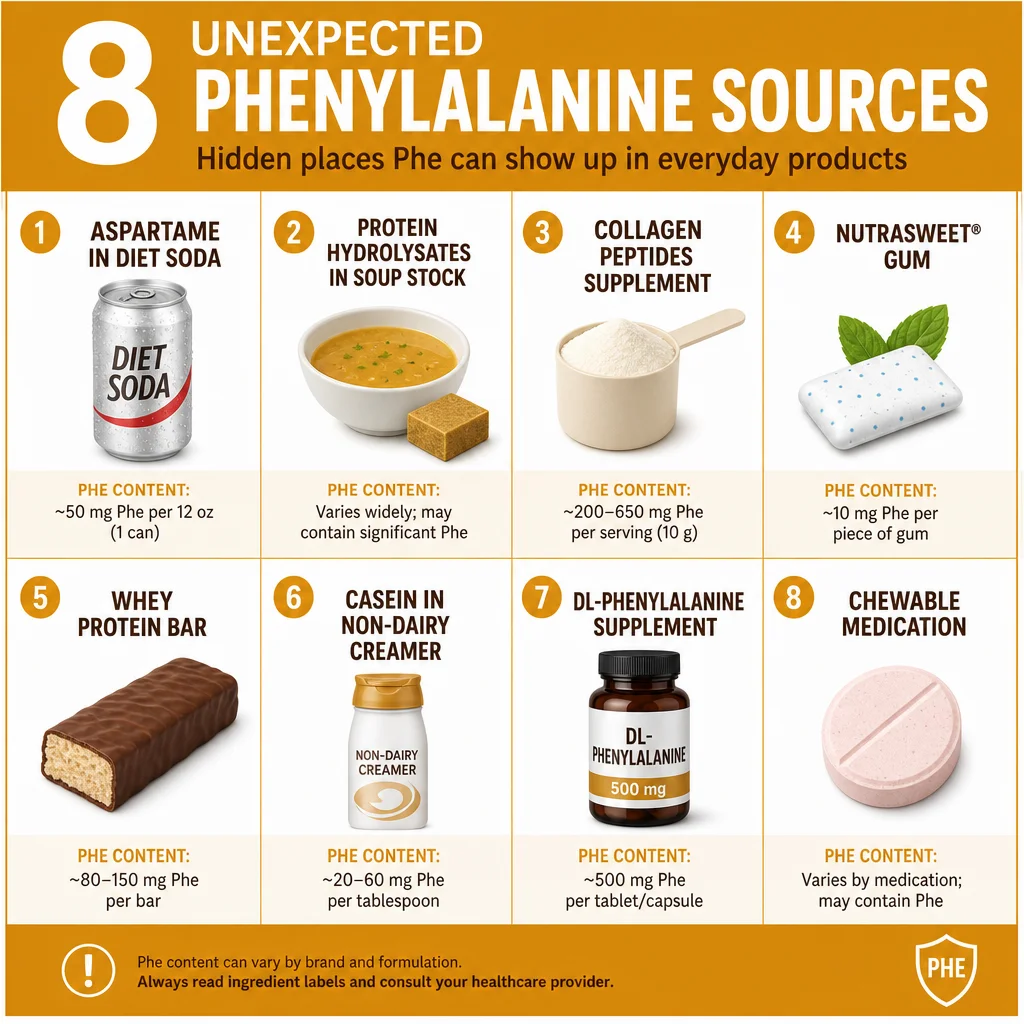
Beyond aspartame, PKU patients must recognize all of the following as significant Phe sources:
Protein hydrolysates: Hydrolyzed vegetable protein (HVP), hydrolyzed soy protein, hydrolyzed wheat protein, and autolyzed yeast extract are all protein fragments containing free amino acids, including phenylalanine. These appear widely in soups, broths, bouillon, savory snacks, sauces, gravies, processed meats, and instant noodles.
Collagen peptides and gelatin: Collagen supplements have become mainstream in wellness products, protein powders, and bone broth products. Collagen contains phenylalanine, though at lower levels than muscle protein. Gelatin, used in marshmallows, gummy candies, Jell-O, and some yogurts, is derived from collagen and carries Phe.
Casein and caseinates: Casein is the dominant milk protein (approximately 80 percent of milk protein). It appears in non-dairy creamers, processed cheeses, and some commercial breads as sodium caseinate or calcium caseinate. Unlike lactose-free dairy alternatives, caseinate-containing products carry significant Phe.
Whey protein: Found in protein bars, protein powders, some breads, and fortified foods. Whey protein concentrate, isolate, and hydrolysate all contain substantial Phe. Even trace amounts added for "protein enrichment" count against the daily budget.
L-Phenylalanine supplements: Products marketed for mood support, pain management, or athletic performance may contain DL-phenylalanine (DLPA) or L-phenylalanine as declared ingredients. These are pure phenylalanine, an acute hazard for PKU patients. Sports supplements and "pre-workout" formulas containing amino acid blends must be individually checked.
Medications containing aspartame: Chewable tablets, orally disintegrating tablets (ODTs), liquid medications, and some vitamins use aspartame as a sweetener. Children's chewable vitamins, antacid tablets, and some prescription medications may contain aspartame without a prominent warning on the dispensing label. Pharmacists should be consulted about inactive (excipient) ingredients.
Natural flavors from protein sources: The regulatory category "natural flavors" can legally include protein-derived compounds. Yeast extracts and meat-based natural flavors may contribute trace Phe. For patients with very tight budgets (under 200 mg/day), even trace sources warrant investigation.