The insulin-driving ingredient on most packaged food labels does not appear simply as "sugar." Here is what to scan for instead.
"-ose" sugars: glucose, dextrose, fructose, sucrose, maltose, lactose, galactose, trehalose, xylose
Syrups: high-fructose corn syrup (HFCS), corn syrup, rice syrup, malt syrup, golden syrup, agave nectar, maple syrup, date syrup, tapioca syrup, sorghum syrup, carob syrup, barley malt syrup
Concentrated fruit forms: evaporated cane juice, fruit juice concentrate, white grape juice concentrate, apple juice concentrate, cane juice crystals
Natural-sounding sugars: coconut sugar, palm sugar, date sugar, molasses, blackstrap molasses, raw sugar, turbinado, demerara, muscovado, sucanat, panela, rapadura, jaggery, honey
Processed derivatives: invert sugar, invert syrup, caramel, refiners syrup, confectioner's sugar
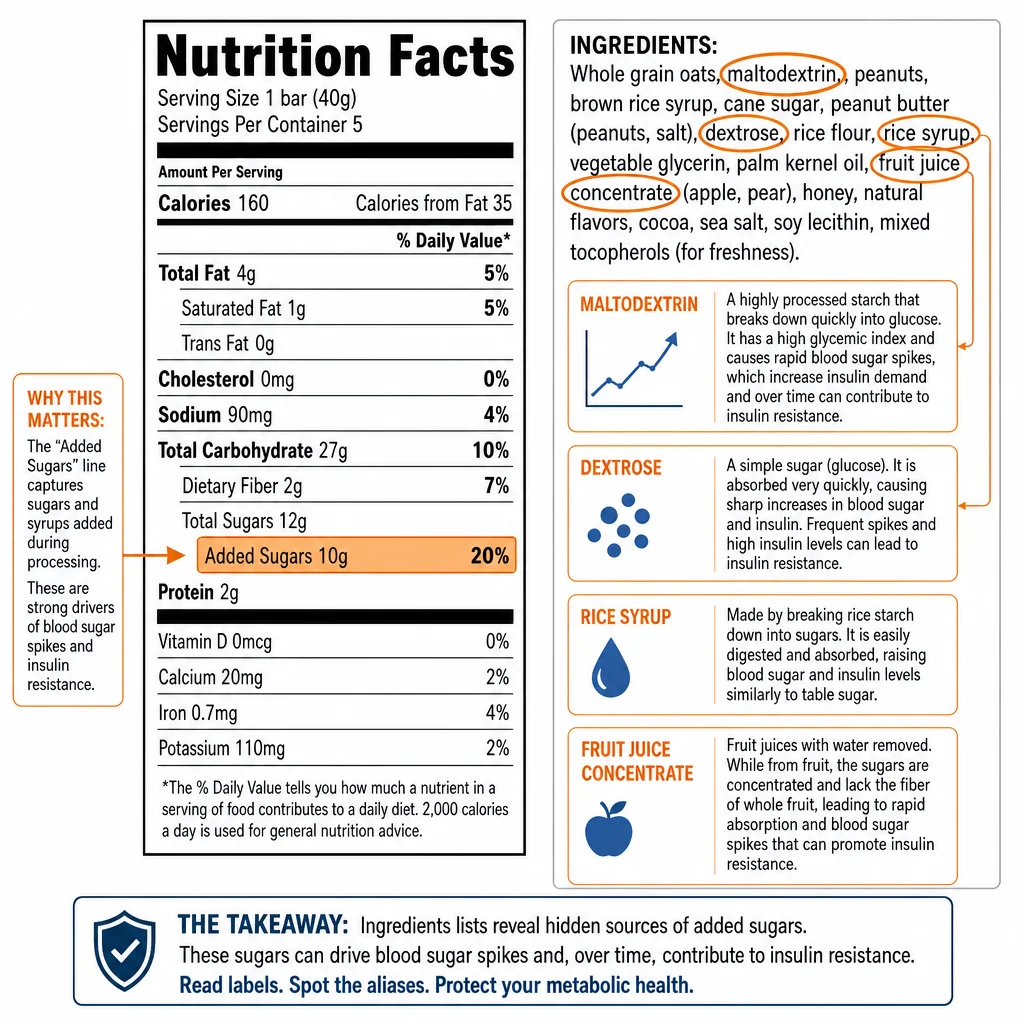
High-glycemic starch derivatives: maltodextrin (GI approximately 110, higher than table sugar), modified corn starch, dextrin, corn syrup solids, these frequently appear in products marketed as "sugar-free"
Since January 2020, FDA has required US manufacturers to list "Added Sugars" as a separate line on the Nutrition Facts panel, beneath Total Sugars. This is the single most reliable data point for PCOS label reading. The American Heart Association recommends women target under 25 grams of added sugars per day. Many flavored yogurts, protein bars, granolas, and cereals marketed as healthy exceed this in a single serving.
Advanced Glycation End Products: The Hidden Insulin Disruptor
Sugar does damage beyond raising insulin acutely. Advanced glycation end products (AGEs) form when sugars react with proteins and fats during the high-heat industrial processing used to make ultra-processed foods, frying, baking at scale, extrusion. A product can appear low in sugar on the label yet still carry a substantial AGE burden if it is heavily processed.
AGEs bind RAGE receptors and activate NF-κB-mediated inflammation and oxidative stress. In PCOS specifically, reducing dietary AGE intake was shown to significantly lower insulin resistance markers and androgen levels in clinical research published in Hormones and Human Reproduction. The practical implication: whole foods prepared simply, even at high temperatures, generate fewer AGEs than industrially produced food-like products.