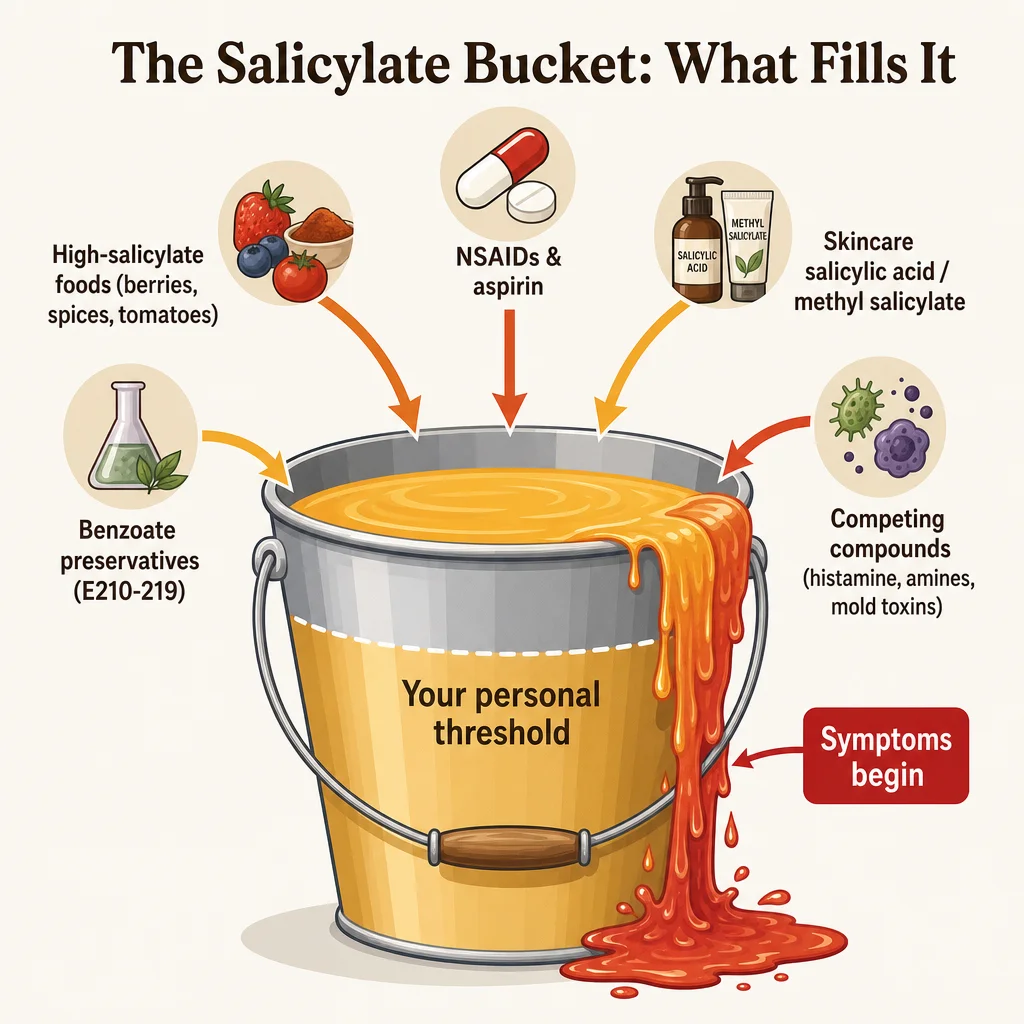
Everyone has a threshold. For some people, a blueberry smoothie and a tomato sauce on the same day crosses it. For others, years of eating berries, spices, and wine cause no problems until gut inflammation, an antibiotic course, or prolonged stress shifts their baseline. Salicylate sensitivity is not all-or-nothing, and that variability is exactly what makes it hard to understand and harder to diagnose.
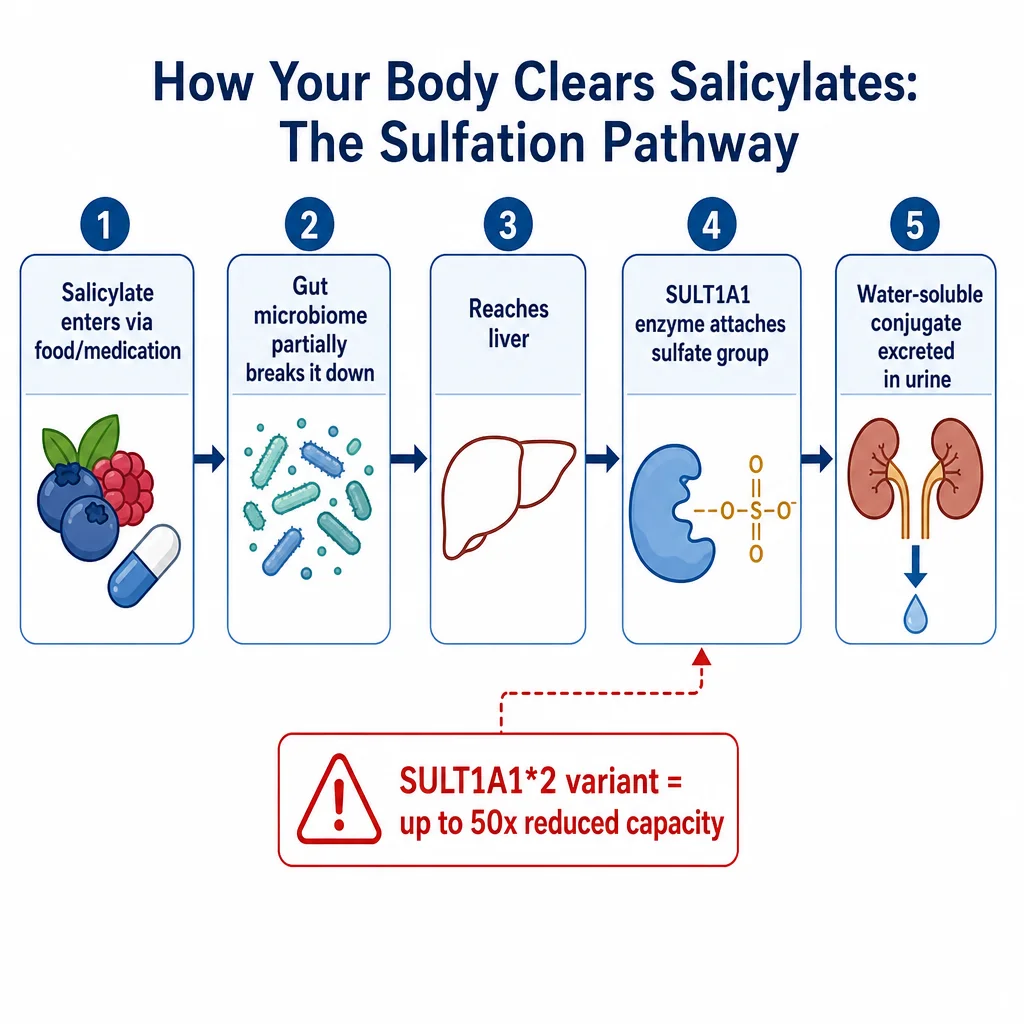
The explanation for why some people react to salicylates and others don't comes down to two compounding factors: how efficiently your liver enzymes can clear salicylates, and what your gut bacteria are doing with them before they get there. Both are shaped by genes, lifestyle, and conditions you may already have.