Salicylates are produced by plants as a defense mechanism against pathogens, insects, and physical damage. Any plant food contains some amount, but concentrations vary widely by species, part of the plant, and ripeness.
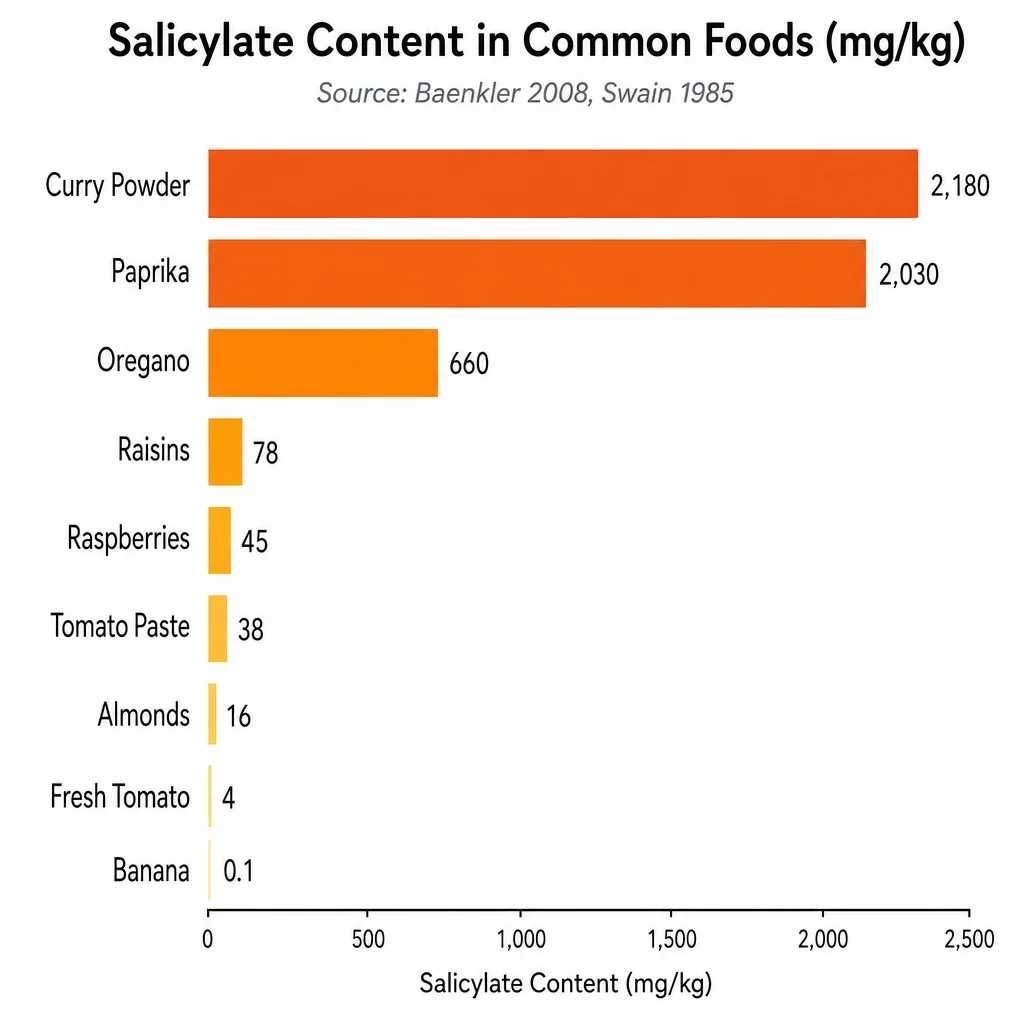
Spices carry the highest concentrations by far. Curry powder comes in at approximately 2,180 mg per kilogram. Paprika sits at 2,030 mg/kg. Oregano, cumin, cinnamon, cloves, turmeric, and rosemary all fall into the very-high category. A single gram of curry powder contains enough salicylate to matter for highly sensitive individuals.
Dried and concentrated fruit forms are next. Raisins, currants, and dried apricots are significantly higher than their fresh counterparts because salicylates concentrate when water is removed. Fresh berries, particularly blackberries, raspberries, blueberries, and strawberries, are also consistently rated high across food composition databases.
Condiments derived from concentrated plant sources carry a risk that is easy to miss. Tomato paste, Worcestershire sauce, and many commercially prepared sauces fall into the high-salicylate category even when the quantity per serving seems small.
Lower-risk foods that reliably appear safe across clinical databases include peeled potatoes, bananas, peeled pears, plain meats and fish, eggs, milk, plain rice, and most legumes. Peeling produce matters: the skin and outer leaves of most fruits and vegetables carry the highest salicylate concentrations.